"Testicle Pain"
Answer: Testicular Hydrocele
Well you guessed it, it is a large testicular hydrocele. The first image shows the large anechoic hydrocele. The second and third images show good color flow around and in the testicle using power doppler.
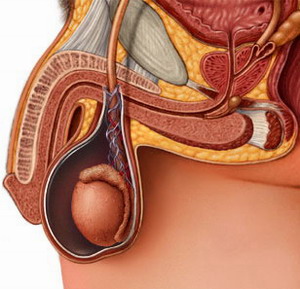
Hydrocele: A hydrocele is an abnormal fluid collection that fills a potential space between the visceral and parietal layers of the tunica vaginalis. Usually they are observed anterolaterally in the scrotum and are not always unilateral. Causes of hydrocele include congenital communications with the abdominal cavity, radiation treament to the testicles, trauma, tumor, testicular torsion or infection. Hydroceles can be communicating or non-communicating, dependent on if there is a channel contiguous with the abdominal cavity.
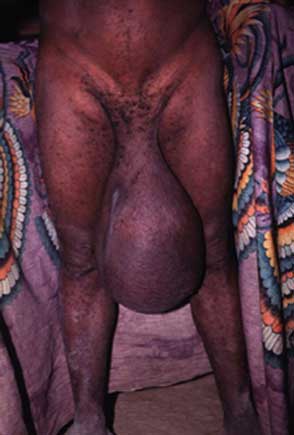
A New Guinea Man with Massive Hydrocele
Varicocele: This entitiy is actually a pathologic engorgement of the pampiniform plexus of veins in the spermatic cord. Varicoceles frequently reduce sperm motility and count, and need surgical correction in some males prior to trying to conceive. Nearly 100% of varicoceles are left sided due to the venous drainage location of the left testicle (i.e. at a 90 degree angle into the left renal artery making presence of a valve nearly impossible. Sonographically they appear as a collection of tube-like structures outside of the testicle (bag of worms-remember?).
A hydrocele will vary in appearance from a varicocele in that the fluid will be completely anechoic and NOT resemble a collection of engorged veins on ultrasound. Further, there will usually be color flow through a varicocele; this is augmented with a valsalva maneuver. Use spectral doppler (pulse wave) and color doppler to ensure no flow is in an area you are diagnosing as hydrocele!
Hematocele: A hematocele is simply a variant of a hydrocele, except the potential space contains some or all blood products -- you can differentiate this by sometimes seeing a slightly more echogenic fluid collection on the monitor representative of the blood or inflammatory cells present in the fluid. A history of testicular or abdominal trauma would heighten the suspicion for a hematocele.
Testicular Torsion: Torsion of the testicle is a feared diagnosis of many EP's due to its association with litigation. Torsion usually occurs secondary to trauma of the testicle or physical exertion (heavy lifting). Laxity in the spermatic cord is the mechanism by which the testicle is allowed to torse in the scrotum, and complete arterial occlusion occurs at 450-540 degrees of rotation. The testicle will become edematous after complete occlusion and no doppler signals will be apparent. If identified within 3 hours a 100% recovery rate is reported, and if identified in 10 hours, an approximate 70% recovery rate is reported.
With our new machines, and power doppler capability, testicular flow is easily achieved. However, for absolute assurance that no torsion is present, we must also employ pulse wave doppler of both the arterial system and venous system in the testicle. This too is not difficult, but takes practice to be proficient. Appearance of the normal uninvolved testicle is key for comparison. Absence of flow on power doppler is highly suggestive of torsion; moreover, lack of venous flow on pulse wave doppler is an early sign of torsion, and lack of arterial waveforms using pulse wave doppler represents frank torsion with certain ischemia. Bedside serial exams can be helpful for determining cases of early torsion that may be evolving.
For now at least, in any man presenting with acute or subacute testicular pain, continue to perform an official ultrasound examination, as some diagnosed cases of epididymitis, varicocele and hydrocele are actually found to be atypical testicular torsion presentations. Maintain a high degree of suspicion in all testicular pain patients.
Good luck, and catch me at any time for help.
Thanks for looking,
Hunter
Back Home
|